Tamika

Clinical description
Tamika is an 11 year old African American female in regular education. Her mother sought treatment for her increased anger, aggression, being “hyper,” having trouble sleeping, lying, talking to herself, and stealing. At home, she was often cranky and refused to share things with her two siblings and younger cousin, who were all living in the same house. When she had tantrums, she screamed, threw things, broke a plate and some toys, and escalated to the point that the mother worried she might injure someone. Tamika is starting to have problems at school, including lower grades and disruptive classroom behaviors such as talking out of turn, getting easily distracted, and frequently arguing with peers and some teachers.
| Extended content |
|---|
History of presenting problemConceptualizationInitial treatment plan |
Assessment findings
Checklist scores
Tamika, her mother, and her teacher all completed the Achenbach System of Empirically Based Assessment (ASEBA) checklists. Here are the results, reported as T scores (M = 50, standard deviation (SD) = 10, compared to other women between 11 and 18 years of age).
| Scale | Mom | Tamika | Teacher |
|---|---|---|---|
| Externalizing | 82 | 75 | 56 |
| Internalizing | 70 | 66 | 54 |
| Anxious/Depressed | 60 | 64 | 59 |
| Withdrawn | 64 | 61 | 50 |
| Somatic Complaints | 76 | 68 | 50 |
| Attention Problems | 68 | 66 | 63 |
| Social Problems | 74 | 73 | 50 |
| Thought Problems | 75 | 70 | 57 |
| Delinquent/Rule-Breaking | 76 | 53 | 50 |
| Aggressive Behavior | 91 | 54 | 59 |
| Extended content |
|---|
|
Select more specialized scales to refine probabilitiesUpdating probabilitiesCritical items |
Diagnostic interview findings
Diagnoses are based on a LEAD (Longitudinal expert evaluation of all data) consensus meeting following a Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS) interview, using DSM-IV criteria. The same interviewer met with Tamika, and then her mother, then discussed any differences of opinion with them as needed to use clinical judgment. KSADS results were reviewed with a licensed clinical psychologist to arrive at a final decision.
- PTSD (100% confidence post interview)
- ADHD (65% confidence post interview)
- ODD (70% confidence post interview)
- Rule out: reactive attachment disorder (49% confidence post interview)
- Rule out: mood NOS (33% confidence post interview)
Cognitive and achievement testing
(Not done as part of the evaluation; may be able to match up information later)
Prediction phase
Let's see how we would apply the EBA principles to Tamika.
Shortlist of probable hypotheses
Based on Tamika's age and the common clinical issues, here are the possible issues:
- Oppositional defiant disorder is a leading hypothesis, based on her high externalizing scores across different reporting groups, and especially from her mother. It also is common.
- Conduct problems would be a second possible diagnosis.
- Attention problems are worth evaluating based on prevalence, though her prior academic performance does not suggest any additional reason for concern.
- Post traumatic stress disorder would be worth considering based on prevalence; nothing immediately suggests it in the presenting problem, but it could explain a similar set of symptoms.
- Parent-child conflict or an adolescent acting out in a somewhat chaotic home environment also should be a contending hypothesis.
Risk and protective factors and moderators
Tamika's gender and age make her on the bubble between oppositional defiant disorder and conduct disorder, for which she is on the younger side of the range.
Updating probability of diagnoses
Below is a worksheet with the DLRs left blank to be filled in. Answers are below.
| Tamika | Common Dx Hypotheses (A) | Starting Prob. (B) | Broad Measure (D) | Cross-informant (E) | Confirmation (G) | Treatment Phase (I), (J), (K) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Base Rate from Rettew et al. (2009) SDI[1] | Scale & Score | DLR | Revised Prob. | EAY Check | Next Test score | DLR | Revised Prob. | K-SADS Interview | |||
| Any Anxiety | Specific Phobia | 0.15 | |||||||||
| PTSD | 0.09 | PTSD (100%) | |||||||||
| GAD | 0.10 | CBCL T
Internalizing 70 |
Other measures are better than Achenbach | ||||||||
| Panic Disorder | 0.11 | ||||||||||
| Social Phobia | 0.20 | ||||||||||
| Separation Anxiety | 0.18 | ||||||||||
| Any Impulse Control Disorder | ODD | 0.38 | CBCL T
Aggressive 91 |
No data about TRF scales for aggressive | ODD (70%) | ||||||
| CD | 0.25 | CBCL T
Aggressive 91 |
|||||||||
| ADHD | 0.38 | CBCL T
Attention 68 |
TRF T
Attention 63 |
0.73 | 0.76 | ADHD combined (65%) | |||||
| Any Mood Disorder | MDD | 0.26 | CBCL T
Anx/Dep 60 |
Haven't found data about TRF for internalizing | |||||||
| BP | |||||||||||
| Dysthymia | 0.08 | ||||||||||
| Any Substance Abuse Disorder | 0.30 | CBCL #2
CBCL #99 CBCL #105 |
|||||||||
Click below for filled out chart.
| Answers | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cross-informant perspectives
Mention that these have DLRs. Also unpack the implications of agreement and disagreement for the client (and add a section about treatment implications of disagreement on the Conceptual Model Pages)
Prescription phase
Mental status and clinical observations
(add content)
Genogram and family functioning
Here is a genogram of Tamika's family:
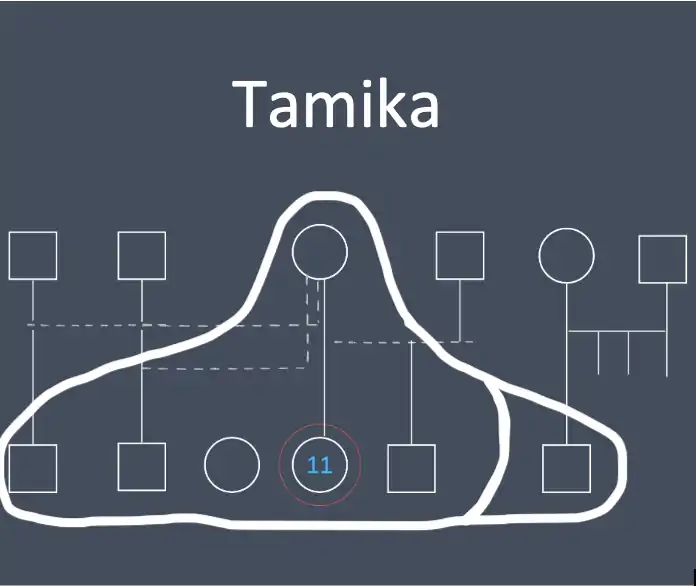
Mom is effectively a single parent raising Tamika and three brothers and a sister. The kids have three different fathers; none of them are currently in the home or contributing directly to child support. On the other hand, there is not any significant conflict with Tamika's father, and she sees him intermittently.
The plot twist hinges around the "uncle" who is shown as being both in and out of the house. Skip to the diagnostic interview section if you want the details.
Treatment selection
The diagnostic interview suggests a combination of a major depressive episode and a prior dysthymia, sometimes referred to as a "double depression." This suggests that Arlene's stress and mood problems have persisted for a long time, and may be more difficult to treat. The mood disorders clearly are associated with impairment and should be a major focus of treatment.
Moderating factors
The double depression is a moderating factor suggesting worse prognosis, along with potential demoralization and early drop out from treatment.
Client preferences
Arlene was originally leaning towards an antidepressant medication, thinking that she could take it without telling her parents. After discussing the pros and cons of medication (including the effect size in youths, the potential side effects, and the fact that her parents would find out as part of the consent process), as well as the pros and cons of different evidence based therapies, she elected to try IPT. She wanted to revisit the possibility of a stimulant helping with her inattention, but she opted to wait and see if that improved along with her mood if the IPT helped.
Process phase
Clinically significant change
Reliable change index
Pick a treatment target and specify what the RCI would be for it. Discuss how you would explain to Arlene.
Given Arlene's main diagnosis with a combination of a major depressive episode and a prior dysthymia, bringing down her depressive symptoms back
Nomothetic benchmarks
A, B, Cs of Jacobson definitions. General stuff about limitations would go on the main concept page. Here it is focused on the client -- what are the benchmarks they will focus on? How explained to them?
Interpreting benchmarks
Minimum important difference (MID)
Note that this section is a dangler -- not originally called out in the 12 steps. Medium d as a rule of thumb from Streiner, Norman, & Cairney (2015). Could work from AUC to d to raw units as a way of estimating, since psychology hasn't done research on this yet. Might be able to back into it with studies that had CSQ and outcome data.
Client goals & tracking
These would be personal goals and idiographic measurement -- YTOPS, etc.
Process measures
This would be traces such as coming to sessions, doing homework assignments. (Not sure of other specifics involved in current IPT protocols?)
Progress measures
YTOPS again and goal setting.
Termination planning and maintenance
Revisit Jacobson benchmarks. Is there much chance of relapse? What things would the client need to pay attention to if they were going to nip that in the bud?
References
- 1 2 Rettew, David C.; Lynch, Alicia Doyle; Achenbach, Thomas M.; Dumenci, Levent; Ivanova, Masha Y. (2009-09-01). "Meta-analyses of agreement between diagnoses made from clinical evaluations and standardized diagnostic interviews". International Journal of Methods in Psychiatric Research 18 (3): 169–184. doi:10.1002/mpr.289. ISSN 1557-0657. PMID 19701924. https://www.ncbi.nlm.nih.gov/pubmed/19701924.