| Subject classification: this is a psychology resource. |
Christopher
Clinical description
Christopher is a 14-year-old White male who lives with his mother and older brother. He is in the accelerated track of courses and skipped a grade. He had been outgoing and popular, and frequently hangs out with his older brother’s friends. He started “hooking up” with women who were friends or acquaintances of his brother. Last year his behavior changed in several ways. He started listening to different music, especially heavy metal, and grunge music. He started dressing differently, wearing spiked leather armbands and boots. Mother reports that he started “hooking” up with girls last year, including older girls who are friends with his older brother. Mom has not confronted him directly about this but believes that he has become sexually active. He has started missing school, sometimes for weeks at a time, complaining of feeling tired and ill, but tests have ruled out bacterial infection and been inconclusive about mononucleosis. The school system has threatened to fail him in all classes for the quarter unless the family can provide a medical explanation for his absences or get him to return to school consistently.
| Extended content |
|---|
History of presenting problemConceptualizationInitial treatment plan |
Assessment findings
Checklist scores
Christopher, his mother, and his social studies teacher all completed the Achenbach System of Empirically Based Assessment (ASEBA) checklists. Here are the results, reported as T scores (M = 50, SD = 10, compared to other males between 11 and 18 years of age).
| Scale | Mom | Christopher | Teacher |
|---|---|---|---|
| Externalizing | 58 | 53 | 42 |
| Internalizing | 54 | 54 | 56 |
| Anxious/Depressed | 60 | 54 | 54 |
| Withdrawn | 50 | 54 | 50 |
| Somatic Complaints | 54 | 55 | 65 |
| Attention Problems | 86 | 73 | 53 |
| Social Problems | 51 | 54 | 55 |
| Thought Problems | 63 | 70 | 57 |
| Delinquent/Rule-Breaking | 57 | 53 | 50 |
| Aggressive Behavior | 58 | 54 | 50 |
| Extended content |
|---|
Select more specialized scales to refine probabilitiesUpdating probabilitiesCritical items |
Diagnostic interview findings
Diagnoses are based on a LEAD (longitudinal expert evaluation of all data) consensus meeting following a Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS) interview, using DSM-IV criteria. The same interviewer met with Christopher and then his mother, then discussed any differences of opinion with them as needed to use clinical judgment. KSADS results were reviewed with a licensed clinical psychologist to arrive at a final decision.
- Bipolar I (85% confidence)
- Specific phobia - animals (90% confidence)
- ADHD combined (70% confidence)
- Rule out chronic tic (45% confidence)
- Rule out Learning Disability not otherwise specified (30% confidence)
Cognitive and achievement testing
(Not done as part of the evaluation; may be able to match up information later)
Prediction phase
Let's see how we would apply the EBA principles to Christopher:
Shortlist of probable hypotheses
Based on Christopher's age and the common clinical issues, here are some possible issues:
- A mood disorder definitely is a leading hypothesis. Within the "mood" category, the hypotheses should consider major depression, dysthymia, and bipolar spectrum disorders, as well as other medical issues that could lead to mood symptoms.
- Substance misuse should be another hypothesis, based again on its prevalence in his age group.
- Conduct problems would be a fourth -- they are not immediately suggested by the description of the presenting problem, but they are common in the age group, and they also can be a risk factor for self harm.
- Attention problems are worth evaluating based on prevalence, though his prior academic performance does not suggest any additional reason for concern.
Risk and protective factors and moderators
Christopher's age increases the probability of a mood disorder, as well as substance misuse, and could be consistent with an adolescent-onset conduct disorder. His solid academic performance previously suggests potential resilience.
Updating probability of diagnoses
Below is a worksheet with the DLRs left blank to be filled in. Answers are below.
| Christopher | Common Dx Hypotheses (A) | Starting Prob. (B) | Broad Measure (D) | Cross-informant (E) | Confirmation (G) | Treatment Phase (I), (J), (K) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Base Rate from Merikangas et al. (2010) NCS-A[1] | Scale & Score | DLR | Revised Prob. | EAY Check | Next Test score | DLR | Revised Prob. | Next Test score | DLR | Revised Prob. | K-SADS Interview | |||
| Any Anxiety | Specific Phobia | 0.19 | Specific Phobia - animals (90%) | |||||||||||
| PTSD | 0.05 | |||||||||||||
| GAD | 0.02 | CBCL T | Other measures are better than Achenbach | |||||||||||
| Panic Disorder | 0.02 | |||||||||||||
| Social Phobia | 0.09 | |||||||||||||
| Separation Anxiety | 0.08 | |||||||||||||
| Any Impulse Control Disorder | ODD | 0.13 | CBCL T
Aggressive 58 |
No data about TRF scales for aggressive | ||||||||||
| CD | 0.07 | CBCL T
Aggressive 58 |
||||||||||||
| ADHD | 0.09 | CBCL T
Attention 86 |
TRF T
Attention 53 |
ADHD combined (70%) | ||||||||||
| Any Mood Disorder | MDD | 0.12 | CBCL T
Anx/Dep 60 |
Haven't found data about TRF for internalizing | ||||||||||
| BP | 0.03 | CBCL T | YSR T
Externalizing 53 |
TRF T
Externalizing 42 |
Bipolar I (85%) | 7 Up 7 Down Inventory (Christopher) | ||||||||
| CMRS-10(Parent) | ||||||||||||||
| Dysthymia | Included above | |||||||||||||
| Any Substance Abuse Disorder | 0.11 | CBCL #2 CBCL #99 CBCL #105 | ||||||||||||
| Answers | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cross-informant perspectives
Mention that these have DLRs. Also unpack the implications of agreement and disagreement for the client (and add a section about treatment implications of disagreement on the Conceptual Model Pages)
Prescription phase
Mental status and clinical observations
(add content)
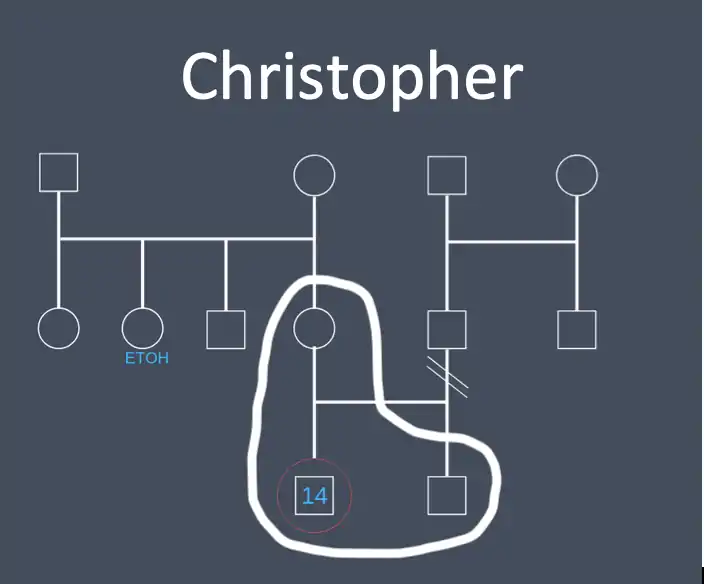
Genogram and family functioning
Here is a genogram of Christopher's family:
Treatment selection
The diagnostic interview suggests found evidence of a prior manic episode, indicating a diagnosis of bipolar I. This suggests that the periods of low energy and cognitive functioning could be depressive episodes, and interviewing confirmed that they would meet diagnostic criteria for a major depressive episode even though Christopher did not describe himself as "depressed." They clearly were associated with impairment and should be a major focus of treatment.
Moderating factors
Client preferences
***
Process phase
Clinically significant change
Reliable change index
Pick a treatment target and specify what the RCI would be for it. Discuss how you would explain to Christopher.
The treatment target we picked was the self-report of attention problems. For reliable change to be demonstrated with 95% confidence, a decrease of 9 points to 62 would have to be seen.
Nomothetic benchmarks
A, B, Cs of Jacobson definitions. General stuff about limitations would go on the main concept page. Here it is focused on the client -- what are the benchmarks they will focus on? How explained to them?
For self report attention problems, to reach the A, B, and C benchmarks, Christopher's scores would have to decrease to:
A- 45
B- 66
C- 58
Interpreting benchmarks
Minimum important difference (MID)
Note that this section is a dangler -- not originally called out in the 12 steps. Medium d as a rule of thumb from Streiner, Norman, & Cairney (2015). Could work from AUC to d to raw units as a way of estimating, since psychology hasn't done research on this yet. Might be able to back into it with studies that had CSQ and outcome data.
Client goals & tracking
These would be personal goals and idiographic measurement -- YTOPS, etc.
Process measures
This would be traces such as coming to sessions, doing homework assignments. (Not sure of other specifics involved in current IPT protocols?)
Progress measures
YTOPS again and goal setting.
Termination planning and maintenance
Revisit Jacobson benchmarks. Is there much chance of relapse? What things would the client need to pay attention to if they were going to nip that in the bud?|}
References
- 1 2 Merikangas, Kathleen Ries; He, Jian-ping; Burstein, Marcy; Swanson, Sonja A.; Avenevoli, Shelli; Cui, Lihong; Benjet, Corina; Georgiades, Katholiki et al.. "Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A)". Journal of the American Academy of Child & Adolescent Psychiatry 49 (10): 980–989. doi:10.1016/j.jaac.2010.05.017. PMID 20855043. PMC PMC2946114. https://dx.doi.org/10.1016/j.jaac.2010.05.017.