Arlene

Clinical description
Arlene is a 16 year old Hispanic female who lives with her mother, father, and three siblings (a sister who is four years older and now in college, and a brother 1 year younger and sister two years younger). She is in regular education classes, and had been an A & B student until this year. Her self esteem has seemed more low this year, and her last marking period she had her lowest grades ever. She becomes angry when pressed about her grades, screaming and storming into the bedroom and locking everyone out for hours at a time. Her parents do not want her dating. However, she has a boyfriend and has been sneaking out of the house late at night to spend time with him. Her father caught her, and there was a massive argument. That weekend, she took a bottle full of approximately 200 aspirin, but then she made herself throw up. She has not talked with her parents about this, but did call her older sister, who encouraged her to talk with the school counselor that had been supportive of the sister.
| Extended content |
|---|
History of presenting problemConceptualizationInitial treatment plan |
Assessment findings
Checklist scores
Arlene, her mother, and her social studies teacher all completed the Achenbach System of Empirically Based Assessment (ASEBA) checklists. Here are the results, reported as T scores (M = 50, standard deviation (SD) = 10, compared to other women between 11 and 18 years of age).
| Scale | Mom | Arlene | Teacher |
|---|---|---|---|
| Externalizing | 67 | 73 | 68 |
| Internalizing | 59 | 68 | 46 |
| Anxious/Depressed | 57 | 62 | 50 |
| Withdrawn | 66 | 68 | 52 |
| Somatic Complaints | 50 | 70 | 50 |
| Attention Problems | 62 | 68 | 58 |
| Social Problems | 61 | 63 | 62 |
| Thought Problems | 55 | 64 | 50 |
| Delinquent/Rule-Breaking | 62 | 70 | 65 |
| Aggressive Behavior | 69 | 72 | 68 |
| Extended content |
|---|
Select more specialized scales to refine probabilitiesUpdating probabilitiesCritical items |
Diagnostic interview findings
Diagnoses are based on a LEAD (Longitudinal expert evaluation of all data) consensus meeting following a Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS) interview, using DSM-IV criteria. The same interviewer met with Arlene and then her mother, then discussed any differences of opinion with them as needed to use clinical judgment. KSADS results were reviewed with a licensed clinical psychologist to arrive at a final decision.
- Major Depressive Disorder (85% confidence post interview)
- Dysthymic Disorder (85% confidence)
- ADHD Inattentive (75% confidence)
- ODD (70% confidence)
- Anxiety NOS (65% confidence)
- Rule out: panic without agoraphobia (45% confidence)
Cognitive and achievement testing
(Not done as part of the evaluation; may be able to match up information later)
Prediction phase
Let's see how we would apply the EBA principles to Arlene:
Shortlist of probable hypotheses
Based on Arlene's age and the common clinical issues, here are the possible issues:
- A mood disorder definitely is a leading hypothesis. The suicide attempt also suggests evaluating mood disorder (although not everyone who attempts suicide has a mood disorder). Within the "mood" category, the hypotheses should consider major depression, dysthymia, and bipolar spectrum disorders, as well as other medical issues that could lead to mood symptoms.
- Substance misuse should be another hypothesis, based again on its prevalence in her age group.
- Anxiety disorders would be a third hypothesis.
- Conduct problems would be a fourth -- they are not immediately suggested by the description of the presenting problem, but they are common in the age group, and they also can be a risk factor for self harm.
- Attention problems are worth evaluating based on prevalence, though her prior academic performance does not suggest any additional reason for concern.
- The family conflict is also important to assess, as well as potential cultural issues (and differences of opinion between Arlene and her parents that might be influenced by differing degrees of acculturation).
Risk and protective factors and moderators
Arlene's gender and age increase the probability of a mood disorder, and may reduce the chances of conduct disorder. Her solid academic performance previously suggests potential resilience.
Her conflict with her father, and her keeping things secret from her parents, would be considerations before doing family therapy, and they may complicate consent for treatment (Arlene is still a minor). Additionally, family relations can impact the development and maintenance of depression. There is a strong link between childhood depression and dysfunction in the family. This would put Arlene at a higher risk for depressive symptoms to maintain if the family dysfunction remains.
Arlene seems to find support from her oldest sister. She could be a good resource for Arlene and could be considered in family therapy.
It would be helpful to know if either of Arlene's parents have a mood disorder. If they do, that would put her at much higher risk for having a mood disorder herself.
Some data suggest that Interpersonal Psychotherapy (IPT) may be particularly effective with Hispanic teens, perhaps moreso than Cognitive Behavioral Therapy (CBT), because of the greater emphasis on family (and familism). IPT would have an advantage of not requiring active participation of the father (unlike family therapy), since IPT is designed as an individual therapy.
Updating probability of diagnoses
Below is a worksheet with the DLRs left blank to be filled in. Answers are below.
| Arlene | Common Dx Hypotheses (A) | Starting Prob. (B) | Broad Measure (D) | Cross-informant (E) | Confirmation (G) | Treatment Phase (I), (J), (K) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Base Rate from Merikangas et al. (2010) NCS-A[1] | Scale & Score | DLR | Revised Prob. | EAY Check | Next Test score | DLR | Revised Prob. | Next Test score | DLR | Revised Prob. | K-SADS Interview | |||
| Any Anxiety | Specific Phobia | 0.19 | Anxiety NOS (65%) | |||||||||||
| PTSD | 0.05 | |||||||||||||
| GAD | 0.02 | CBCL T
Internalizing 59 |
Other measures are better than Achenbach | |||||||||||
| Panic Disorder | 0.02 | |||||||||||||
| Social Phobia | 0.09 | |||||||||||||
| Separation Anxiety | 0.08 | |||||||||||||
| Any Impulse Control Disorder | ODD | 0.13 | CBCL T
Aggressive 69 |
No data about TRF scales for aggressive | ODD (70%) | |||||||||
| CD | 0.07 | CBCL T
Aggressive 69 |
||||||||||||
| ADHD | 0.09 | CBCL T
Attention 62 |
TRF T
Attention 58 |
ADHD inattentive (75%) | ||||||||||
| Any Mood Disorder | MDD | 0.12 | CBCL T
Anx/Dep 57 |
Haven't found data about TRF for internalizing | MDD (85%) | |||||||||
| BP | 0.03 | CBCL T
Externalizing 67 |
YSR T
Externalizing 73 |
TRF T
Externalizing 68 |
Bipolar I (85%) | |||||||||
| Dysthymia | Included above | Dysthymia (85%) | ||||||||||||
| Any Substance Abuse Disorder | 0.11 | CBCL #2
CBCL #99 CBCL #105 |
||||||||||||
| Answers | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Cross-informant perspectives
Mention that these have DLRs. Also unpack the implications of agreement and disagreement for the client (and add a section about treatment implications of disagreement on the Conceptual Model Pages)
Prescription phase
Mental status and clinical observations
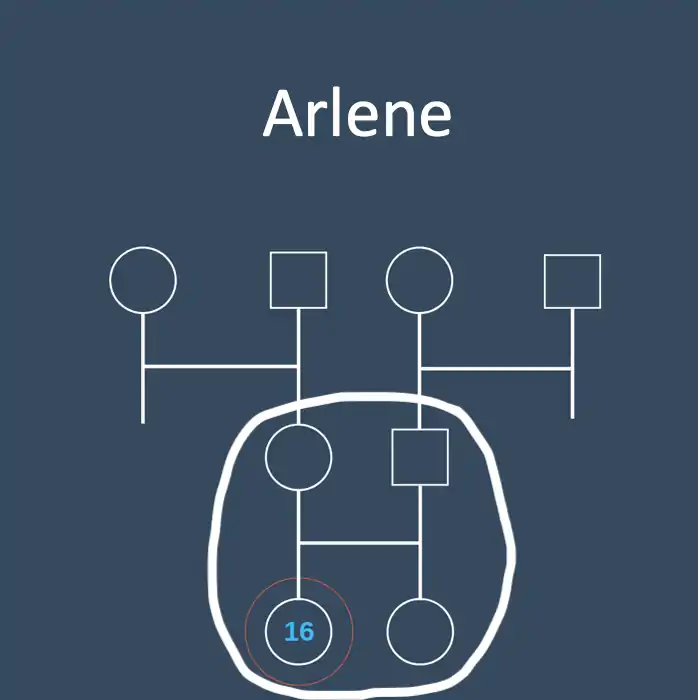
Genogram and family functioning
Here is a genogram of Arlene's family:
Treatment selection
The diagnostic interview suggests a combination of a major depressive episode and a prior dysthymia, sometimes referred to as a "double depression." This suggests that Arlene's stress and mood problems have persisted for a long time, and may be more difficult to treat. The mood disorders clearly are associated with impairment and should be a major focus of treatment.
Cognitive Behavioral Therapy (CBT) is a well-supported treatment option. Interpersonal Psychotherapy for Adolescent Depression (IPT-A) is a good option as well. IPT may be the best option for Arlene, because studies have shown it to be especially effective with Hispanic youth. It places a large emphasis on the adolescent's independence, and focuses on the reciprocal relationship between mood and relationships.
Moderating factors
The double depression is a moderating factor suggesting worse prognosis, along with potential demoralization and early drop out from treatment.
Client preferences
Arlene was originally leaning towards an antidepressant medication, thinking that she could take it without telling her parents. After discussing the pros and cons of medication (including the effect size in youths, the potential side effects, and the fact that her parents would find out as part of the consent process), as well as the pros and cons of different evidence based therapies, she elected to try IPT. She wanted to revisit the possibility of a stimulant helping with her inattention, but she opted to wait and see if that improved along with her mood if the IPT helped.
Process phase
Clinically significant change
Reliable change index
Pick a treatment target and specify what the RCI would be for it. Discuss how you would explain to Arlene
Nomothetic benchmarks
A, B, Cs of Jacobson definitions. General stuff about limitations would go on the main concept page. Here it is focused on the client -- what are the benchmarks they will focus on? How explained to them?
Interpreting benchmarks
Minimum important difference (MID)
Note that this section is a dangler -- not originally called out in the 12 steps. Medium d as a rule of thumb from Streiner, Norman, & Cairney (2015). Could work from AUC to d to raw units as a way of estimating, since psychology hasn't done research on this yet. Might be able to back into it with studies that had CSQ and outcome data.
Client goals & tracking
These would be personal goals and idiographic measurement -- YTOPS, etc.
Process measures
This would be traces such as coming to sessions, doing homework assignments. (Not sure of other specifics involved in current IPT protocols?)
Progress measures
YTOPS again and goal setting.
Termination planning and maintenance
Revisit Jacobson benchmarks. Is there much chance of relapse? What things would the client need to pay attention to if they were going to nip that in the bud?
References
- 1 2 Merikangas, Kathleen Ries; He, Jian-ping; Burstein, Marcy; Swanson, Sonja A.; Avenevoli, Shelli; Cui, Lihong; Benjet, Corina; Georgiades, Katholiki et al.. "Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A)". Journal of the American Academy of Child & Adolescent Psychiatry 49 (10): 980–989. doi:10.1016/j.jaac.2010.05.017. PMID 20855043. PMC PMC2946114. https://dx.doi.org/10.1016/j.jaac.2010.05.017.